New Submissions Are Not Currently Being Accepted
Samples sent after April 10, 2024 will be put on hold.
Viewing desktop version: Switch to Mobile
Heroin Powder (Realdope 31679)
Sold as: Heroin
ID: 3531
| Test Date: | Mar 24, 2015 |
|---|---|
| Pub. Date: | Mar 24, 2015 |
| Src Location: | Online |
| Submitter Loc: | Online, -- United States |
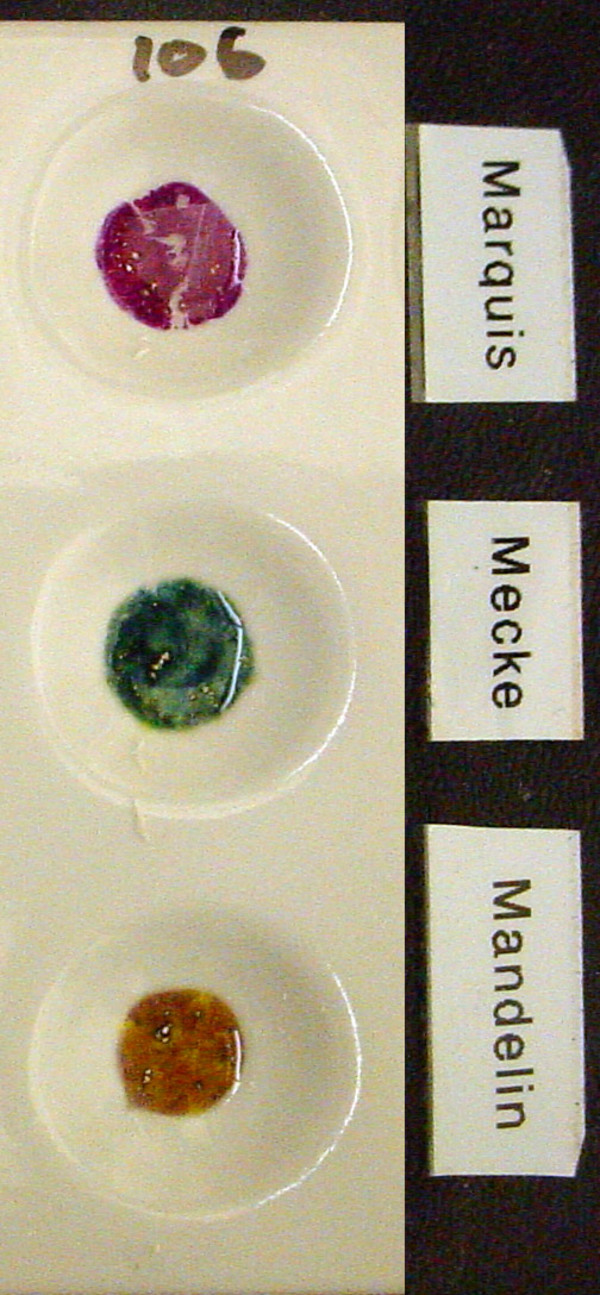
| Color: | Off White / Brown |
| Size: | 400 mg |
| Data Source: | DrugsData (EcstasyData) |
| Tested by: | DDL |
| Lab's ID: | 20150300106 |
Sold as: Heroin
Expected to be: Heroin
6-monoacetylmorphine is quite potent opiate agonist that, like heroin, quickly gets metabolized to morphine. I believe the metabolism of heroin generates either 3-mono or 6-monoacetlymorphine as an intermediary before it is metabolized to morphine. 6MAM is considered 'good stuff' by geeky users, though. Some folks attribute the fact that IV heroin generates the most euphoric opiate high due to the creation of 6MAM. Heroin itself only has a half-life of something like 14 minutes.
Acetylcodeine (aka 6-monoacetylcodeine) is a quite weak opiate, but it does show some binding affinity for the mu receptor, hence analgesia. It has a potency of approximately 1/3 that of codeine. I had to look that one up, see Ansonoff M, Grace R. 'Codeine and 6-acetylcodeine analgesia in mice.' Cellular and Molecular Neurobiology. 11/2006; 26(4-6):1011-9.
The actylcodeine (i.e. 6-monoacetylcodeine) gets rapidly metabolized to codeine, which, in turn, is metabolized into morphine. The reason the acetylcodeine is a problem is due to the fact that you want to avoid IVing the drug. I assume that is due to the same reason you want to avoid IVing codeine (pulmonary edema that can be fatal). I have heard stories about people IVing codeine and being OK, but the medical community sees a huge risk with it. At a minimum though, it causes wicked histamine release and one would probably just get pins and needles.